


障害児者診療について
Medical Care for Special Needs
当院では障害のある方も、検査診療を行っています。
- 手持ちの検査機器で、顎台に顎を載せられない方にも、できるかぎりの検査をします。
- 自閉症のある方は、一般診療の最後(あるいは最初)に診ております(お電話にてご予約をお願いします)。
- 手術加療が必要な場合は、障害児者医療に理解のある洛和会音羽病院アイセンターにて加療を行っております。
障害のある子どもこそ、(眼科)医療が必要です。(雑誌AERAに掲載)
2012年より3年間、奄美大島の障がい児支援団体(NPO法人)より依頼を受け、眼科診療を数か月に一度行いました。14回の訪島で、134名(延べ人数370名)の眼科診療を行い、約半数の子供達に眼鏡処方を行いましたが、次の受診時には表情が変わり、話す言葉も増え、様々なことに興味をもつように変わっていました。
ヒトの見る機能は、8歳ごろまで成長すると言われていますが、実は生後2歳までに感受性が最も強い時期があります。強い遠視や乱視のあるお子様は眼鏡による矯正をできるだけ早く行うことが理想です。しかし視力検査ができるのは一般的にも3歳半以降で、障害を持っていればさらに遅れてしまっているのが現状です。
障害を持つ子供ほど、近視・遠視や乱視の確立が高く、ダウン症児では約7割に眼鏡装用が必要とも言われ、当院では1歳児に眼鏡処方をすることもあります。ものがはっきり見えていれば、子供はいろいろなことにさらに興味を示し、発達全体に大きな影響を与えます。
どうぞお気軽にご相談ください。
自閉症の方の白内障や眼瞼の手術加療も担当医として加療を行っています。
自閉症の方の白内障や眼瞼の手術加療も担当医として加療を行っています。手術加療が必要な方に大きな病院を紹介しても受診が難しい方がおられます。当院では、クリニックで眼科受診に慣れていただき、手術前の検査は最新の機械を備えている病院で負担少なく行い、手術も担当し、術後の通院はクリニックで行っています。
雑誌AERAに掲載
(クリックで拡大)
*English and Korean translations are provided below.
English translation of the magazine “AERA”
Children with Disabilities Often Avoided by Medical Institutions
Becoming ‘Medical Refugees’: Disabled Children Denied Necessary Treatment
Despite the need for medical care, there are reported cases of disabled children being refused treatment. To ensure these children receive appropriate medical attention, the collaboration of medical professionals and guardians, along with proper consideration and preparation, is crucial.
“It’s Impossible Here”: The male doctor visibly displayed an unwilling expression when a 49-year-old woman from Tokyo took her 14-year-old eldest daughter to a local plastic surgery and dermatology clinic. The daughter, who had fallen at home during infancy, had intellectual disabilities and autism spectrum disorder.
Recalling the incident, the woman said, “Perhaps because she was restless, I was told, ‘We can’t examine this kind of child.’ While they might have treated a healthy child, children with disabilities often face difficulties in accessing proper treatment.”
The woman also struggled to find an ophthalmology clinic that would see her daughter. It wasn’t until her daughter turned 11 that they found a clinic where she could undergo a thorough examination, revealing her eyesight was normal. The current challenge they face is dental care. Despite taking her daughter to a reputed dental clinic nearby, she felt that the examinations were conducted reluctantly. Even slight movements during the examination resulted in an immediate end to the process. Despite visits every 2-3 weeks, cavities were overlooked, and her daughter, at one point, became unable to eat due to tooth pain. Consulting another dentist, a male dentist confessed, ‘We’re understaffed, and if she moves during treatment, and I cut the inside of her mouth, I wouldn’t be able to take responsibility.'”
Despite the Claim of “Free Access”
One aspect of Japan’s medical system is the principle of “free access.” According to the Japan Medical Association’s website, it asserts that individuals can “freely get examined and receive medical services (treatment) at any medical institution by any doctor without any restrictions.” However, in reality, due to their unique characteristics, disabled children often face challenges in accessing examinations and treatments at medical institutions, and instances of them being denied medical care exist.
A woman from Yokohama City, whose 9-year-old daughter is in 3rd grade and has cerebral palsy, shares her experience:
“There are many doctors with discriminatory beliefs, leaving me speechless. An ophthalmologist once told my daughter’s friend, ‘Is there any meaning in making glasses for such a severely disabled child?'”
Due to her daughter’s athetoid cerebral palsy, she experiences “involuntary movements” beyond her control. Unfortunately, only a few medical institutions comprehend this condition. In the field of dentistry, where there is specialized care for the disabled, the woman took her daughter due to concerns about her misaligned teeth. However, she was implicitly denied orthodontic treatment, with the explanation, “She’s still one of the better cases among disabled children,” leading her to discontinue the visits.
Time and Energy Needed
“Medical care is particularly crucial for disabled children,” emphasizes Dr. Masami Pak, the director of “Masami Eye Clinic” in Kyoto City. In the field of ophthalmology, disabled children exhibit refractive errors, such as farsightedness or nearsightedness, where the image is not properly focused on the retina, approximately five times more frequently than their healthy counterparts. Dr. Pak stresses that medical examinations are even more imperative for them due to the heightened likelihood of unclear vision.
For the past three years, Dr. Pak would travel to Amami Oshima island in Kagoshima every few months to conduct ophthalmological examinations for disabled children. Those who received prescribed glasses exhibited brighter expressions, spoke more words, and developed an interest in various activities by their next visit. ‘Just with a proper pair of glasses, a child’s life can change, and so can their family’s. I’ve come to realize the transformative impact of such medical care.’
However, she also empathizes with doctors who hesitate to examine disabled children. ‘Examining and treating individuals with disabilities demands significantly more time and energy, and one must possess techniques tailored to each person’s characteristics, along with the understanding of a team of staff.’ As an illustration, three years ago, during her tenure as a part-time doctor at Otowa Hospital Eye Center in Kyoto City, she performed cataract surgery on a 20-year-old intellectually disabled man with autism. The man, being large-built, had lost vision in one eye due to self-harm. Considering the challenges posed by his autism in handling new situations, Dr. Pak took the initiative to explain the examination room, operating room, and hospital ward in advance using photos. Multiple practice sessions under general anesthesia were necessary, requiring him to come for examinations many times. Additionally, to prevent infection post-surgery, the standard hospitalization period of 1-2 days was extended to two weeks. The ward nurses conducted study sessions on autism, and the hospital made necessary preparations to accommodate his unique needs.”
Explaining Using Picture Cards
Associate Professor Toshiaki Suwa from Kawasaki University of Medical Welfare, an expert in disability support, points out:
“Unlike visible physical disabilities, intellectual disabilities and autism spectrum disorders are often encountered without proper consideration, with an attitude of ‘conform to normal people’s standards.’ Due to the characteristics of their disabilities, verbal explanations are challenging to comprehend, and they struggle to articulate their symptoms. Difficulty in foreseeing events leads to disruptions in waiting and examination rooms due to their inability to endure the uncertainty. Sensory hypersensitivity requires special consideration during treatment. Developing systems, such as providing incentives through fee schedule points for preparation before treatment, could encourage more medical institutions to accept such patients.”
At Asahide Child Education Institute, a private special needs school in Nerima Ward, Tokyo, they have supported hospital visits for ophthalmology, dentistry, otolaryngology, and other specialties for the past four years. Collaborating with the school doctor, they take photos in advance of the hospital entrance, reception desk, examination room, and treatment equipment. They explain the examination procedures using photo cards, setting individualized small step goals for each student. For students sensitive around their ears, they start by touching their ears with a cotton swab and gradually progress to using tweezers as preparation for treatment. Initially, the students are accompanied on visits, and as they become more accustomed, the family takes over.
A high school boy with Down syndrome, who initially ran around the school to avoid going to the dentist, can now go independently, manage payment, and return home after three years. An elementary school child with autism spectrum disorder, who visited the school dentist every three months, has learned to visit a neighborhood dentist near his home.
Obligation for Reasonable Accommodation
The school initiated examination visit support after school nurse Haname Okada’s distressing experience. She accompanied a female junior high student with autism spectrum disorder, injured in the eye during class, to visit an ophthalmologist. The male doctor instructed them to “Look inside the machine,” but the student couldn’t comply. Frustratingly, the doctor yelled, “I don’t need money, so go home!” leaving Okada-san in tears. She emphasizes, “Because they have disabilities, sometimes they cannot be conscious of taking care of their own bodies, so they especially need medical care. However, there are limits to understanding doctors. I want them to accumulate experiences of hospital visits gradually so they can receive appropriate treatment when it matters.”
Last year, the Act to Eliminate Discrimination against Disabled Persons was revised, making reasonable accommodation obligatory for private businesses, including medical institutions, by June 2024. What kind of support is necessary for hospital visits?
Associate Professor Rika Tsubomi from Hamamatsu University School of Medicine, co-author of the “Support Book for Nurses and Healthcare Staff for Treating Children with Developmental Disability Tendencies,” explains:
“It is not appropriate for nurses to restrain a crying or disruptive child with several people. Medical professionals should gather information from guardians about the child’s difficulties due to their characteristics and past medical experiences. They should convey, in simple words and as briefly as possible, what experiences the child will have.”
Co-author Associate Professor Tomomi Mizuno from the University of Tsukuba emphasizes that preparation on the parents’ side is also crucial. “If a child is deceived into going to a medical institution, they will form a negative impression, making subsequent visits even more challenging. Showing photos of the medical facility and doctors from their website and explaining the examination contents using picture cards beforehand allows the child to mentally prepare, reducing their anxiety.”
Korean translation of the magazine “AERA”
AERA 2022年1月17日 No.2 P.62-63
의료기관에서 멀리하는 경향이 있는 장애를 가진 아이들
장애아동들이 ‘의료난민’이 되다
장애아동이야말로 의료가 필요하지만, 진료를 거부 당하는 경우도 있다고 한다.
적절한 의료 혜택을 제공 받기 위해서는 의료관계자나 보호자들의 배려와 준비가 중요하다.
“아~ 우리는 무리,무리예요.”
남성의사가 누가 봐도 싫은 듯한 표정을 보였다. 도쿄의 중심 지역의 여성(49)의 장녀가 유아기에 집에서 넘어져서 이마가 찢어져, 동네의 ‘형성외과・피부과’ 클리닉에 데려갔을 때의 일이다. 장녀는 지적 장애를 가진 자폐 스펙트럼증이다. 여성은 이렇게 회고한다. “침착하지 않기 때문에 이런 아이는 (이마를) 못 꿰맨다고 들었습니다. 장애를 가지지 않는 아이라면 해주었다고 생각하지만 장애아동은 제대로 된 치료를 못 받을 때가 많아요.”
안과에서도 진료를 받을 수 있는 곳을 찾지 못해 장녀가 11살이 되었을 때 처음으로 문제 없이 보인다는 것을 알 수 있었다. 지금 가장 고민인 것은 치과이다. 동네에서 평판이 좋은 클리닉에 장녀를 데리고 갔지만, 마지못해 진료하고 있는 느낌을 받았다. 기구를 입에 넣어 조금이라도 몸을 움직이면 바로 (진료가) 종료되었다. 2, 3주에 한 번 정도로 치과에 다녔으나 충치가 있는 것도 확인해주지 않아 장녀는 이가 아파서 한동안 식사를 못했다. 다른 치과의원에 상담하니, 남성치과의는 “일할 사람은 모자라고 치료중에 움직여서 입 안에 상처라도 나면 책임을 질 수 없다.” 고 본심을 이야기해주었다.
프리 액세스인데
일본의 의료제도의 특징 중 하나는 ‘프리 액세스’. 일본의료회 홈페이지에는 ‘어떤 제한도 받지 않고 어느 의료기관에서도, 어느 의사에게도 자유롭게 진료를 받을 수 있고 의료서비스(치료)를 받을 수 있다’고 되어 있으나, 현실은 장애아동은 그 특성으로 인해 의료기관에서의 진료나 치료를 받기 어렵고, 진료를 거부 당하는 경우도 있다.
뇌성마비인 초등학교 3학년의 딸(9)이 있는 요코하마시의 여성도 이렇게 이야기한다.
“의사 중에는 차별적인 생각을 가진 사람이 많아서 말이 안 나와요. 딸의 친구는 안과의에게서 ‘이런 중도장애아동에게 안경을 만들 의미가 있나요.’라는 말을 들었습니다.”
딸은 뇌성마비 무정위형(Athetoid type)이기 때문에 자기 의사와는 관계없이 ‘불수의 운동’을 동반하나, 이해해주는 의료기관은 많지 않다고 한다. 치과에는 ‘장애자치과’가 있기 때문에 치아의 배열이 신경 쓰여서 진료를 받았지만 “장애아동 치고는 아직 고른 편이니까요.”라고 은근히 교정치료를 거부 당해, 치과에 다니는 것을 그만 두었다.
시간과 에너지 필요
“장애를 가진 아이야말로 의료가 필요합니다,”
이렇게 말하는 것은 교토시의 ‘마사미안과클리닉’(まさみ眼科クリニック)의 원장, 박마사미의사이다. 안과영역에서는 장애아동은 비장애아동과 비교하여 망막증에 초점이 맞지 않는 원시나 근시 등의 굴절 이상이 약 5배 많아, 분명하게 보이지 않을 가능성이 높기 때문에 진찰이 보다 필요하다고 강조한다.
과거에 박씨는 3년간 몇개월에 한 번, 가고시마의 아마미오시마(奄美大島)에 가서 장애아동의 안과진료를 했었다. 안경을 처방해준 아이들은 재진료 때 표정이 밝아져, 말도 많아지고 여러가지 일에 흥미를 가지게 되었다.
“(아이에게)맞는 안경 하나로 그 아이의 인생이 바뀌고 가족의 인생도 바뀐다. 이런 의료가 있다는 것을 배웠습니다.”
한편, 장애아동의 진료를 멀리하는 경향이 있는 의사들의 사정도 이해가 된다.
“장애아동의 진료는 몇 배나 되는 시간과 에너지가 필요한 데다가 개개인의 특성에 맞춰진 기술이나 많은 스텝들의 이해도 필요합니다.”
예를 들어 3년 전에 비상근 (파트타임) 의사로 근무하는 오토와병원아이센터(音羽病院アイセンター)에서 지적장애와 자폐증을 가진 20살 남성의 백내장수술을 했을 때의 일이다. 남성은 몸집이 크고 한쪽 눈은 자상(自傷)으로 인해 실명되었었다. 자폐증의 특성으로 처음으로 겪은 경험을 싫어하기 때문에 진료실이나 수술실, 입원병동의 사진을 미리 찍어서 설명해, 전신마취의 도입 연습만으로도 여러 차례의 진료가 필요했다. 또한 보통 1박2일의 입원기간을 2주로 하고 병동 간호사들은 자폐증에 대한 공부를 하기 위한 스터디를 여는 등, 병원 측도 받아들이는 태세를 갖추었다.
그림 카드로 설명하다
장애자지원에 대해 잘 아는 가와사키의료복지대학(川崎医療福祉大学) 스와 도시아키씨는 이렇게 이야기한다.
“지체 부자유의 경우와는 달리, 장애가 주변에 잘 보이지 않는 자폐증이나 지적 장애면 배려도 안하고 “보통 사람의 기준에 맞추세요”라고 되기 쉽습니다. 장애의 특성으로서, 말로 하는 설명을 잘 이해하지 못하고 자신의 증상도 잘 전할 수 없고, 앞일을 예측하는 것이 어렵기 때문에 못 참고 대합실이나 진찰실에서 소란을 피워 버립니다. 감각 과민증이 있는 경우는 치료에도 배려가 필요합니다. 치료 전 준비과정에도 진료 보수 점수를 매기는 등 제도를 정비하면 받아들이는 의료 기관도 늘어나지 않을까요.”
도쿄도 네리마구에 있는 사립 특별지원학교인 아사히데학원(旭出学園)에는 4년 전부터 치과와 안과, 이비과 등의 의료기관에서의 진료를 서포트하고 있다. 학교의에게 협력을 얻어 사전에 의원 현관이나 접수처, 진찰실, 치료에 쓰이는 기구 등의 사진을 촬영하여 그림카드도 사용하여 진료 순서를 설명한다. 한 명 한 명에게 스몰 스텝으로 목표를 설정한다. 귀 주변의 과민성이 높은 학생에게는 면봉으로 귀를 만져보고, 괜찮으면 다음에는 핀셋으로 한 단계 높여 치료를 향해 준비한다. 진료에도 동반하여 적응이 되면 가족끼리 통원하도록 한다.
고등부에 다니는 다운증후군인 남학생은 처음에는 치과에 데리고 가려고 하면 학교 안을 도망 다녔지만 3년 걸려서 혼자서 치과에 가서 계산도 마치고 돌아올 수 있는 단계가 되었다. 학교의의 치과에 3개월에 한 번 통원하던 초등부 아동은 자택 근처의 치과에도 다닐 수 있게 되었다.
합리적 배려의 의무화
아사히데학원이 진료 서포트를 시작한 것은 양호 교사인 오카다 하나에씨의 쓴 경험이 계기가 되었다고 한다.
수업 중에 눈을 다친 자폐 스펙트럼을 가진 중등부의 여학생과 함께 안과 진료를 받았을 때의 일이었다. 남성의사가 “기계 안을 들여다보라”고 했지만, 학생을 그러지 못했다. 그러자 의사는 “돈은 필요없으니까 돌아가라”고 소리쳐, 오카다씨는 분해서 눈물을 흘리며 돌아왔다고 한다.
“장애가 있으면 자기가 자기 몸을 가누자는 의식을 가질 수 없을 때도 있어서 보다 의료가 필요하지만 이해해주는 의사선생님은 한정되어있어요. 만일의 경우에 적절한 치료를 받을 수 있도록 조금씩이라도 진료 경험을 쌓아줬으면 좋겠어요.”
장애자차별해소법이 작년에 개정되어, 2024년6월까지 의료기관을 포함한 민간사업자에게도 합리적배려가 의무화된다. (장애아동이) 진료를 받을 때 어떤 지원이 필요한가.
‘간호사・의료스텝을 위한 발달장애 경향이 있는 아이들의 진료서포트북’공저자인 하마마쓰의과대학(浜松医科大学) 준교수 쓰보미 리카씨는 이렇게 이야기한다.
“불안함이나 망설임 때문에 울거나 소란을 피우는 아이를 간호사 여러 명이 붙잡고 억누르는 것은 적절한 대응이 아닙니다. 의료자 측은 아이에게 무엇이 괴로운지 하는 특성과 과거의 진료 체험에 대해서 보호자로부터 정보를 수집하여, 아이가 무엇을 체험할지 최대한 짧고 간단한 언어로 전달해 주세요.”
동저의 공저자인 쓰쿠바대학 준교수 미즈노 토모미씨는 보호자 측의 준비도 중요하다고 강조한다.
“(아이를) 속여서 의료기관에 데려가면 아이에게 의료기관에 대한 나쁜 인상을 심어 다음 진료가 더욱 힘들어집니다. 홈페이지를 활용해서 사전에 의료기관이나 의사의 사진을 보여주거나, 그림카드로 진료내용을 사전에 전해두면 아이는 마음의 준비를 해둘 수 있고 불안함을 경감시킬 수 있습니다.”
P.62 오른쪽 하단 이미지
‘장애자치과’도 있지만 대부분 진료는 평일이다. 학교를 쉬고 가는 것은 일상이 흩뜨려지는 것에 스트레스를 받는 자폐증을 가진 자들에게는 어렵다고 한다.
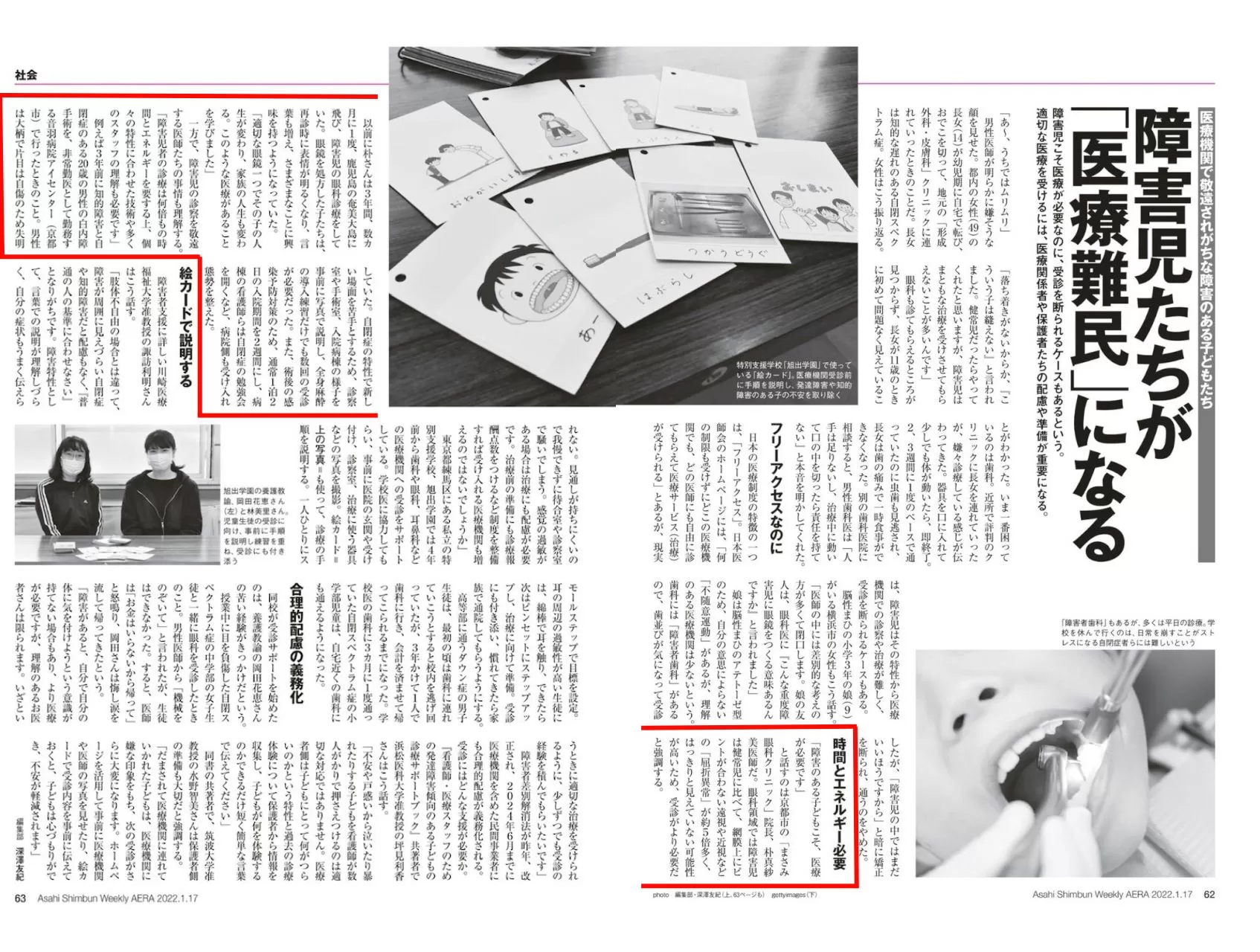
P.62-63 상단 중앙 이미지
특별지원학교‘아사히데학원’에서 사용하는 ‘그림카드’. 의료기관에서 진료 받기 전에 순서를 설명하고 발달장애나 지적장애가 있는 아이의 불안함을 없앤다.
P.63 왼쪽 중앙 이미지
아사히데학원 양호교사, 오카다 하나에씨(왼쪽)과 하야시 미사토씨. 아동학생의 진료를 위해 사전에 순서를 설명하고 연습을 거듭해 진료에 동반한다.
障害者の診療
毎年1~5か所の作業所から依頼を受け、眼科検診を担当しています。

